Ch 1-6
Nothing to be explained further.
________________________________________________________________________
Ch 7
*Gastroscopy: Medical intervention that allows a doctor to see inside the stomach via a tube that is inserted through the nose or mouth all the way to the stomach.
(here it was through the mouth: see Ch 8)
________________________________________________________________________
Ch 8
*Chronic gastritis: chronic inflammation to the stomach (due to irritation of the cells), mainly due to toxic substances or drugs. His alcoholism could very well have played a part in this.
*Erosive (1) vs metaplastic (2): (1) = thinning of the layer of cells or mucus of the stomach, making it more vulnerable to irritation, infections and inflammation, which can cause tumors if it isn't stopped; (2) = differentiation of the stomach cells into cells of the intestines (with a different color, therefore visible with gastroscopy): very suspicious: tumors in development!
*Diffuse hyperemic change: Hyperemia = "Active hyperemia is caused by an increased flow of blood into your organs. It usually happens when organs need more blood than usual." - source: https://www.healthline.com/health/hyperemia => this means a part of the stomach has a strong growth of blood vessels; worst case scenario this is linked to tumors (and thus cancer!), but most often it is trivial and not a cause to worry yet.
Diffuse means it is spread rather than very localized.
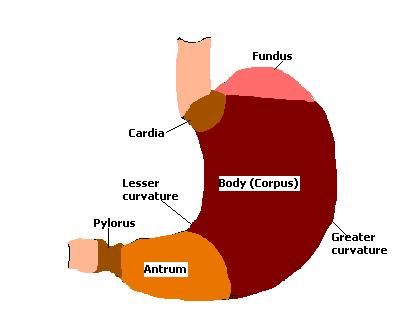
*Antrum: Last part of the stomach, right before the duodenum.
________________________________________________________________________
Ch 31
*Radiation Therapy: using electromagnetic radiation to destroy cancer cells, often gamma rays or X-rays;
*Metastasis: the spreading of tumor cells via the blood circulation, which is severe: new tumors could appear anywhere (but often in the liver);
*Embolism: Blood clot(s) being transported in the blood stream. If they end up stuck in the capillaries (smallest blood vessels) of the lungs they may disable a part of the lungs: very dangerous and can cause several problems with the respiratory system;
*Pneumonia: Lung inflammation (could be due to lack of oxygen because of the embole).
*Phlegm: Mucus (in the lungs), which for instance due to inflammation is more present: water is attracted to the place of inflammation.
---
V. Fib Heart Attack = Ventricular Fibrillation: uncoordinated contractions of the heart causing a heart attack, because the pump function of the heart is compromised. The body will suffer from a lack of oxygen in the tissues, of which most important the brains. Within seconds, the patient loses consciousness and in minutes there is irreversible damage.
*AED will reset the pump function of the heart via an electric shock, mostly started from 200J (lower for children!).
*CPR will manually give a push in the right direction so the tissues can be supplied with little oxygen, all small bits help until the patient can receive an electric shock.
Deadly when not resolved with an AED (electric defibrillator) or AED after delay with CPR ("heart massage").
V-Fib => https://en.wikipedia.org/wiki/Ventricular_fibrillation
AED => https://en.wikipedia.org/wiki/Automated_external_defibrillator
CPR => https://en.wikipedia.org/wiki/Cardiopulmonary_resuscitation
---
Digoxin and Delta Waves:
Delta Waves = "oscillations that predominate in the 1- to 4-Hz range and are commonly referred to as slow wave activity in the EEG." Delta waves are for example picked up by an EEG when someone is in a deep sleep.
EEG = Electroencephalogram (measurement of brain activity). This is not easy to explain and I do not know the relation between delta waves and heart problems, but this site links the effects of digoxin and delta waves (if you press CTRL+F and type "digoxin").
Source: https://www.sciencedirect.com/topics/neuroscience/delta-wave
Digoxin is a very risky drug to use, because of its narrow therapeutic-toxic range. This means a slight overdose can be lethal, and a slight underdosage may end up in therapy failure. For this reason it definitely should not be seen as a first drug to be used! By saying that he should use a Class 1A drug instead, Jin-Hyun means there are better options than Digoxin for slowing down a fibrillating heart (as far as I can see, I think the heart rate is 174! Comparing that to a normal heart rate of 60-100 ish bpm it really is a concern to be handled immediately).
It has positive inotropic and negative chronotropic characteristics on the heart, meaning that it causes the heart to beat with more force (+ inotropic) and slows down the heart rate (- chronotropic). This last feature is used for its normal indications, which are AF (Atrium Fibrillation) and HF (Heart Failure): the atria (upper chambers) are not sending out electric signals to the ventricles (lower chambers) the correct way and so the pump function of the heart is compromised, and the heart rate is sped up; it decreases the norepinephrine levels through activation of the parasympathetic system, and therefore lowers the stress on the heart by slowing it down, which is necessary to calm the heart from the rough strain.
Source: https://go.drugbank.com/drugs/DB00390
However, here the patient is unconscious and already has a high blood pressure (NIBP of 158 is still way above the 130 systolic / 90 diastolic blood pressure) and an elevated heart rate! This means the heart is working way above its capabilities. When not monitored carefully, the following can happen:
"Digoxin poses a risk of rapid ventricular response that can cause ventricular fibrillation in patients with an accessory atrioventricular (AV) pathway. Cardiac arrest as a result of ventricular fibrillation is fatal." - (go.drugbank.com, Digoxin, Pharmacodynamics)
Source: https://www.sciencedirect.com/topics/neuroscience/delta-wave
Source: https://go.drugbank.com/drugs/DB00390
Source: https://www.mayoclinic.org/diseases-conditions/ventricular-fibrillation/symptoms-causes/syc-20364523
---
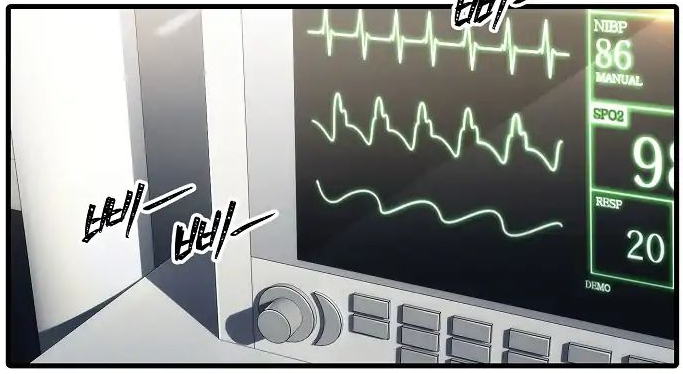
Taking a look at the instrument that checks the critical parameters (heart and lungs function) and displays blood pressure and respiration (Ch 31) is really interesting:
*NIBP = non-invasive blood pressure = blood pressure measured without injection, for instance with a cuff around the arm (but most of the times another external method will be used);
*SPO2 = peripheral blood oxygen saturation => % of hemoglobin that is saturated with O2: the more, the better:: in Ch 67 it is explained that a normal person should have at least 92% saturation;
*RESP: linked to respiration: probably the amount of times the patient breathes per minute while resting/not moving, some sources say it is ~16/min and that it is more healthy the more it is reduced (to 10/min):: here the patient has 20/min which is higher than normal!;
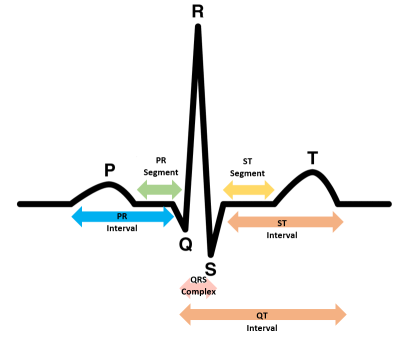
*ECG or EKG (highest graph): pattern of how the heart functions: in this case it is normal and symmetrical. You can clearly see the P-Q-R-S-T repeating waves (see below)
*BP (Blood Pressure graph, middle): Blood Pressure in the heart (and also the arteries to the tissues via the aorta): fluctuation between DBP (diastolic BP = lowest point) and SBP (systolic BP = highest point). There are no mathematical values given so that could've been better ehm.. For a healthy person around 120/80 mm Hg (SBP/DBP) or a bit lower is said to be the desired target, but for many people this will be too hard to reach so then 130/90 is a more realistic target (especially the older the patient).
Sources:
>> https://www.mayoclinic.org/diseases-conditions/high-blood-pressure/in-depth/blood-pressure/art-20050982
>> 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Page 3287 Table 18
*The one at the bottom idk.
________________________________________________________________________
Ch 32
This should be a question about potassium (not calcium, as is shown in wrong translations). Potassium has indeed a possibility to cause heart attacks, but mainly if they are
1) administered using an injection (IV), thus all K+ will be in the bloodstream;
or 2) given to a person whose kidneys are malfunctioning, then the levels of potassium in the blood circulation cannot be regulated as good as in healthy people.
Note that K+ is vital for the normal function of the heart, but that it is dangerous to have too low levels, as well as too high levels, and that the safe range isn't that large. Normally the body uses homeostasis (equilibrium) to balance the intake and excretion of K+ but for example when people inject large doses (which is abnormal, no-one needs K+ injections, K+ pills or foods as bananas are safer) the body can't keep up.
Some numbers to this: It is about very low concentrations:
(K+: ~39 g/mol = 39 mg/mmol)
Normal plasma concentration of K+: min 3.5 - max 5.5 mmol/L = min 136.5 mg/L - max 214.5 mg/L
Hypokalemia = concentration too low: < 3 mmol/L = < 117 mg/L
Hyperkalemia = concentration too high: there are two grades of severity;
1] > 5.5 mmol/L leads to uncoordinated function of the heart;
2] > 8 mmol/L leads to a complete halt of the function of the heart. (> 312 mg/L)
Source: Course Pathophysiology of the human, 2021, University of Ghent
As a person of 70 kg has about 5 liters of blood, you can see that there's not even 2 g of potassium in the blood.
(K+ is also largely present in the fluid inside the cells but here it's not important.)
________________________________________________________________________
Ch 34
lol as if everyone knows what the 5-HT receptor is haha! It's the serotonin neurotransmitter receptor, and serotonin is linked to how one feels (too low concentrations of serotonin in the central nervous system leads to depressions, which they are trying to treat). 5-HT stands for 5-hydroxytryptamine, with tryptamine being the reagent in the formation of serotonin. Multiple neurotransmitter or hormone receptors are directly named after the neurotransmitter/hormone itself, however serotonin is an exception to this.
Other neurotransmitters are Noradrenaline/Norepinephrine (α1, α2, β1, β2 receptors), Dopamine (D receptors) and Acetylcholine (N and M receptors).
Other circulating signal molecules are Adrenaline/Epinephrine (β2 receptors), Histamine (H receptors) and GABA (GABA receptors).
Source: Course Medicinal Chemistry, 2023, University of Ghent
However, neurotransmitters not only situate themselves in the central or periphere nervous system, it can also take place in the GI-tract (Gastro-intestinal tract). Serotonin can be present in the GI-tract as well as in the bloodstream, fulfilling different functions (platelet function, digestive function).
Source:https://en.wikipedia.org/wiki/Prokinetic_agent
"The inhibition of serotonin reuptake can affect platelet aggregation since platelets also express the serotonin transporter. SSRIs (antidepressants such as (es)citalopram can result in decreased storage of serotonin in platelet dense granules. Increased serotonin can also increase gastric acid secretion, which increases the risk for ulceration. SSRIs in combination with NSAIDs (such as ibuprofen, non-opioid painkillers (without paracetamol/acetaminophen) also show a significantly increased risk of upper GI bleeding."
Source:https://pmc.ncbi.nlm.nih.gov/articles/PMC9680839/
________________________________________________________________________
Ch 61
More info about Enoxaparin (LMWH = low molecular weight heparin => involvement in the mechanism causing blood not form thrombi/emboles):
Source: https://go.drugbank.com/drugs/DB01225 or more specific https://go.drugbank.com/drugs/DB01225#mechanism-of-action
Low molecular weight heparins are powerful anticoagulantia administered subcutaneously (see the syringe at the right side) twice a day to prevent the blood from creating blood clots in patients which have a high risk for embolism and cerebrovascular accidents (CVA). Factor Xa, which is an activated clotting factor in the blood (activated => to cause blood to clot; previously unactivated factor X is normally present in the blood ready to be activated when needed) in the formation process of blood clots, is bound to Antithrombin (naturally endogenous in the human body) and the LMWH, which quickly lowers the chances of clots making an appearance.
However, all antithrombotics can cause (severe) bleeding so it isn't without risks.
Source: Course Pharmacology, 2023, University of Ghent
________________________________________________________________________
Ch 73
is rupture of the aorta really 90% of the times fatal? Yes I get it's a super important part of the arterial system but damn that's almost a death warrant; in Ch 75 it's said that the 90% mortality level stays even if a surgeon tries to mend the aneurysm (= rupture due to bursting of a blood vessel).
________________________________________________________________________
Ch 124
*Immunosuppressants are absolutely necessary for people who have undergone an organ transplantation, most often they need to take them for the rest of their life, otherwise the organ might be rejected because it wasn't their own organ and the immune system sees it as something to be removed/destroyed. The only exception would be from twins born from the same egg (need to search proper term, in Dutch it is called "eeneiige tweeling"). This leads to formation of a weaker immune response.
So here the concentration/level needs to be high enough for the liver to keep on working without signs of rejection.
*Obviously, because you suppress the immune system for the organ transplant, the patient is vulnerable for all kinds of infections. Vigilance is required, and check-ups on the patient should be frequent. |